Serpiginous choroiditis

Figure 1. Color retinography of the right eye

Figure 2. Color retinography of the left eye. Both retinographs show serpiginoid peripapillary atrophy without vitreous cellularity.

Figure 3. Right eye autofluorescence: a hyperautofluorescent area adjacent to the atrophic area is observed, which corresponds to an active flare.
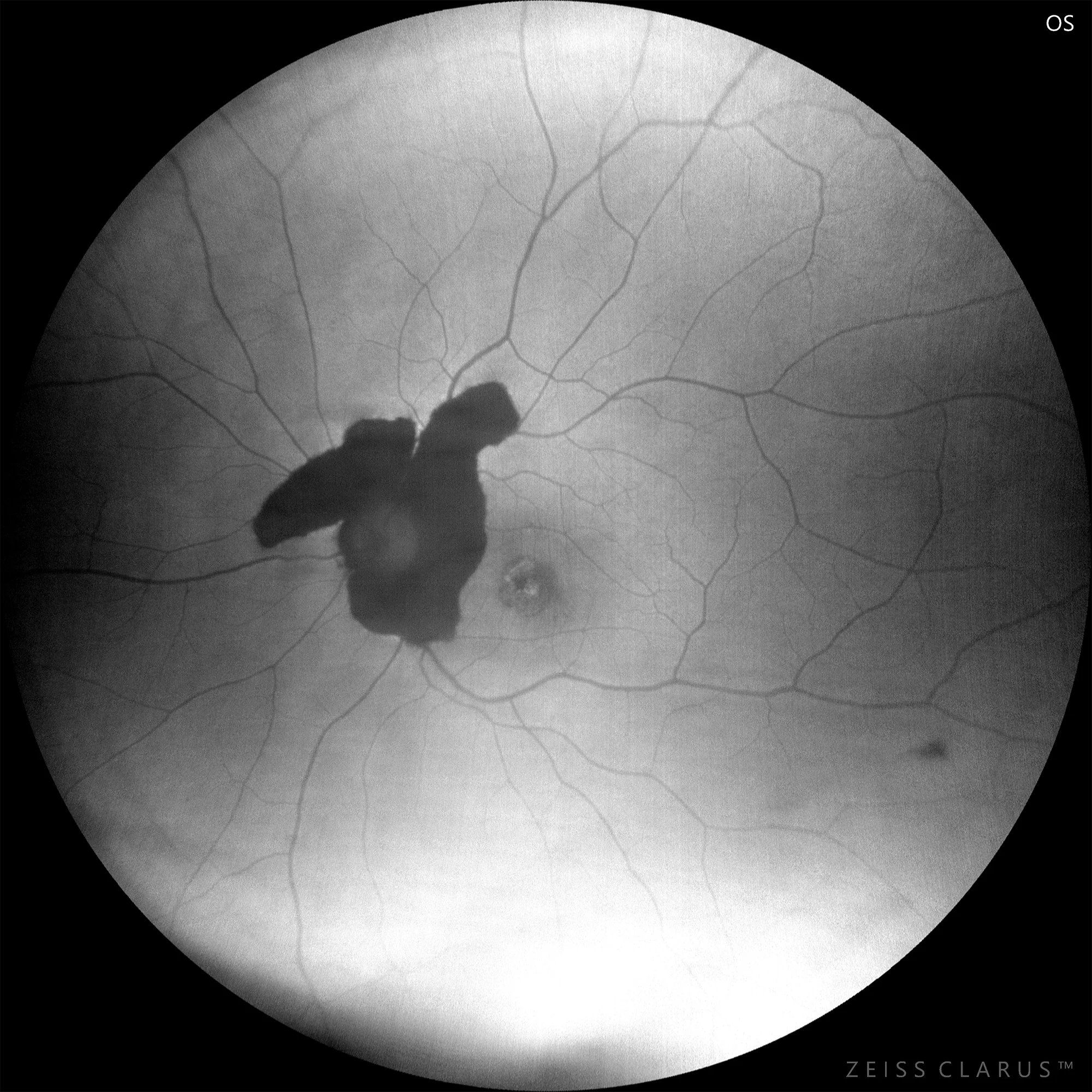
Figure 4. Autofluorescence in the left eye: marked hypoautofluorescence with a characteristic serpiginoid appearance. A foveal lesion is also observed, which corresponds to a neovascular membrane under antiVEGF treatment.
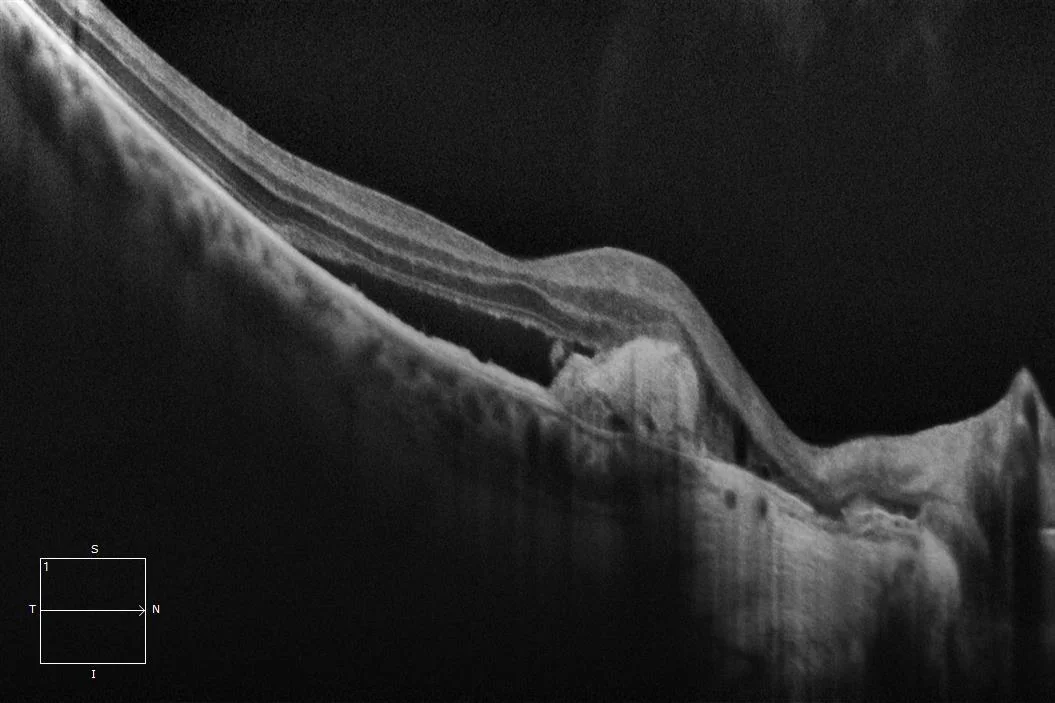
Figure 5. Optical Coherence Tomography of the right macular eye. Neovascular membrane with subretinal fluid adjacent to area of complete peripapillary outer retina atrophy.
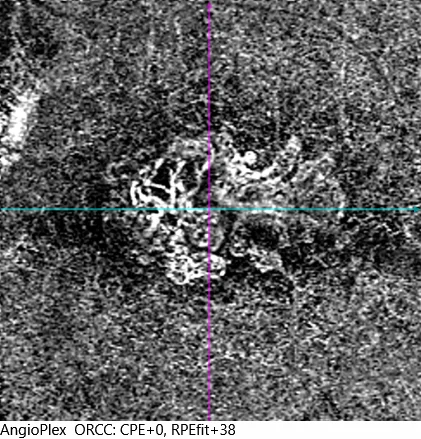
Figure 6. Angio-OCT of the right eye. Choriocapillary ischemia of the affected area is observed with the presence of a neovascular membrane.
Description
Serpiginous choroiditis is a form of choriocapillaritis that affects young men bilaterally. Inflammatory flares that cause ischemia of the choriocapillaris are typical, with a typical appearance of serpentine or serpiginoid atrophy. There is usually no evidence of inflammatory signs such as vitritis, vasculitis or anterior chamber cellularity. The flares leave an atrophic legacy that corresponds to a hypoautofluorescent area in the autofluorescence and complete atrophy of the outer retina in the macular optical coherence tomography (mOCT). In classic serpiginous choroiditis, it is characteristic that the lesion begins in the papillary area and the inflammatory flares originate at the limits of the atrophic area.
To prevent its progression, as in other posterior uveitis, immunosuppressive treatment is often required.
The appearance of neovascular membranes (NVM) at the edges of the lesion is relatively common, and they generally respond well to anti-angiogenic (antiVEGF) treatment.