Acute central serous chorioretinopathy
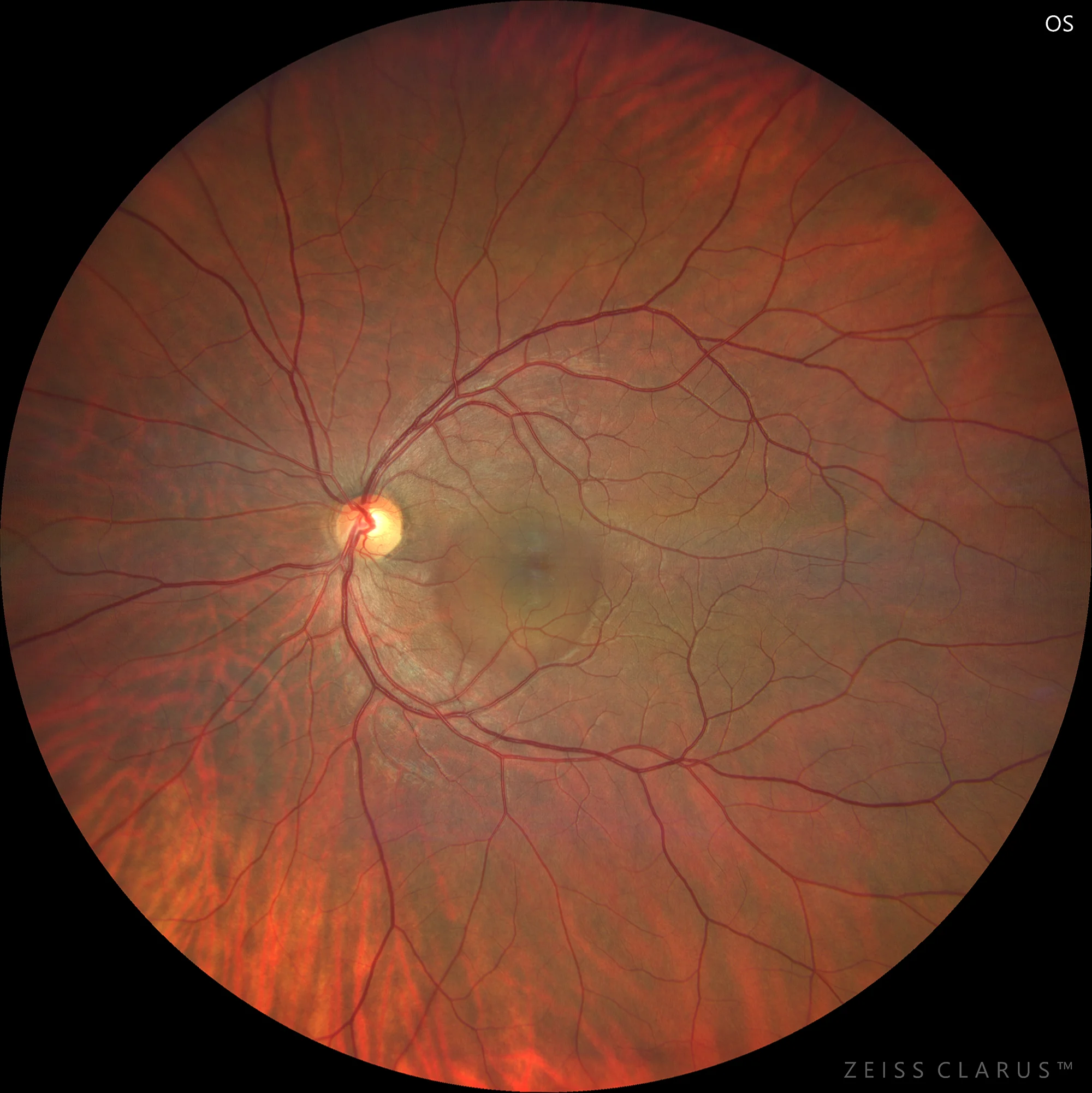
Color retinography showing a retina with little tessellation in the posterior pole, and a transparent blister of subretinal fluid at the macular level.
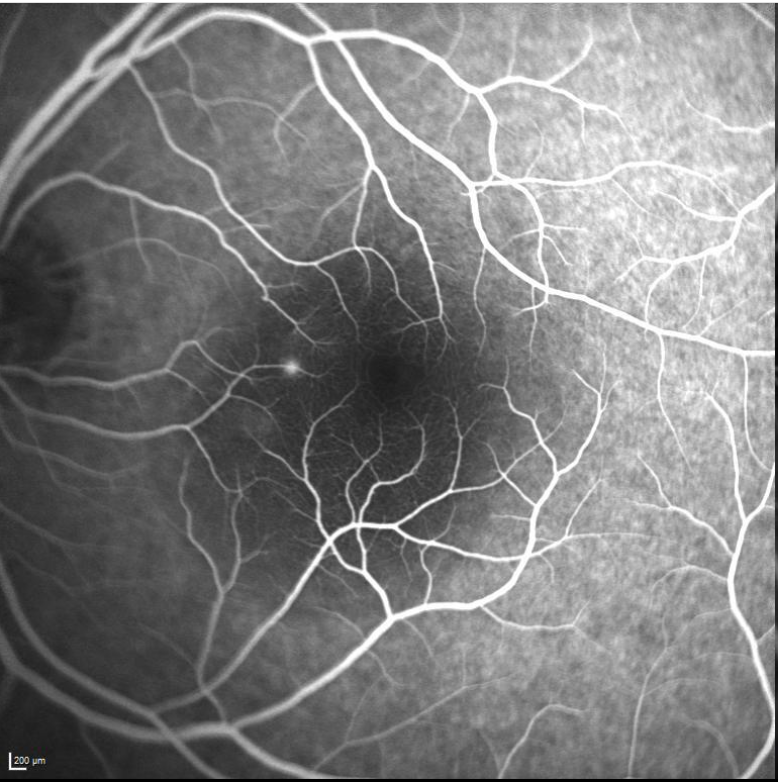
Fluorescein angiography shows normal vascular architecture. Characteristic of this pathology is a leakage point of the nasal dye to the macula with inkblot staining.
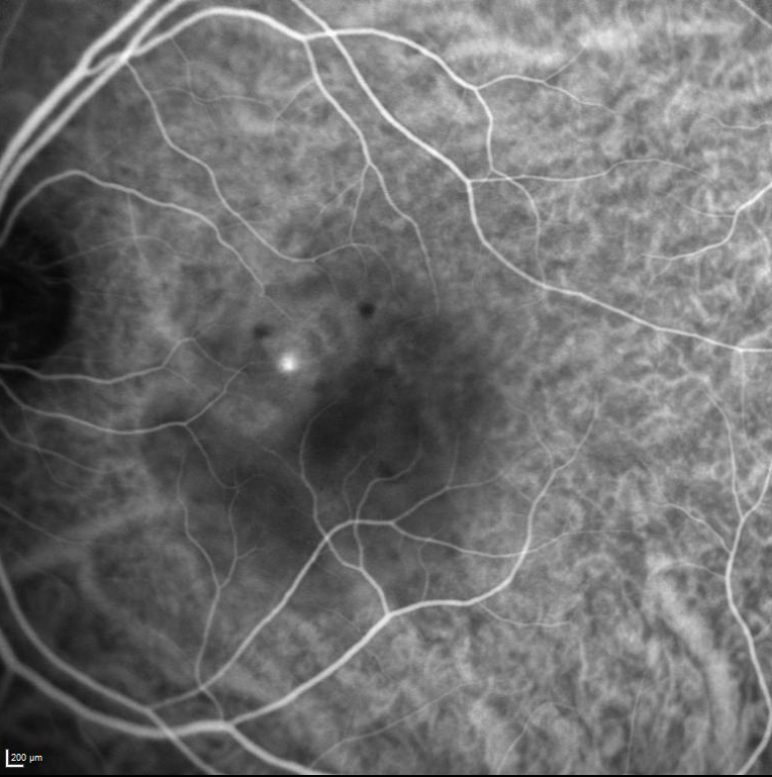
Indocyanine green shows some hypocyanescence, likely secondary to compression of the pachychoroid vessels. The same leakage point observed with fluorescein is also present. It's important to remember that leakage points are not always visible with indocyanine; their appearance depends on the size of the leakage point. Finally, note the hypocyanescent areas secondary to RPE detachments.
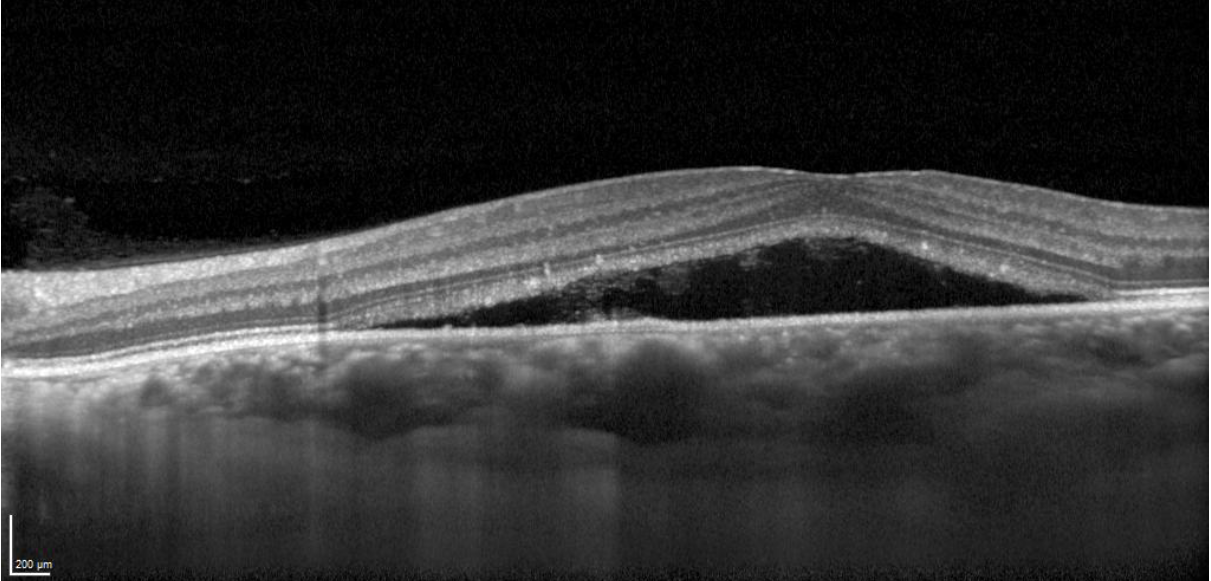
OCT shows a neurosensory retinal detachment. We can see elongation of the photoreceptors, towards the nasal side of the fovea, hyperreflective content in the subretinal space, some excavation on the roof of the elongation of the photoreceptors. And coinciding with the leak point, we detect the presence of a large choriocapillaris vessel compressing the choriocapillaris.
Description
Acute central serous chorioretinopathy. Acute central serous chorioretinopathy (CSCR) is an ocular pathology characterized by the accumulation of serous fluid between the retinal pigment epithelium (RPE) and the neurosensory retina, leading to serous detachment of the macula. This disorder predominantly occurs in young and middle-aged men and is associated with risk factors such as stress, corticosteroid use, and a type A personality profile. The etiology of CSCR is not fully understood, but choroidal hyperpermeability is thought to play a crucial role, facilitated by blood-retinal barrier dysfunction. Patients typically present with blurred vision, metamorphopsia, and micropsia. Diagnosis is confirmed by imaging techniques such as optical coherence tomography (OCT) and fluorescein angiography, which show serous detachment and subretinal fluid leakage. Although CSCR may resolve spontaneously in many cases, treatment may include laser photocoagulation or photodynamic therapy (PDT), or subthreshold laser for chronic or recurrent cases.