Central retinal artery occlusion
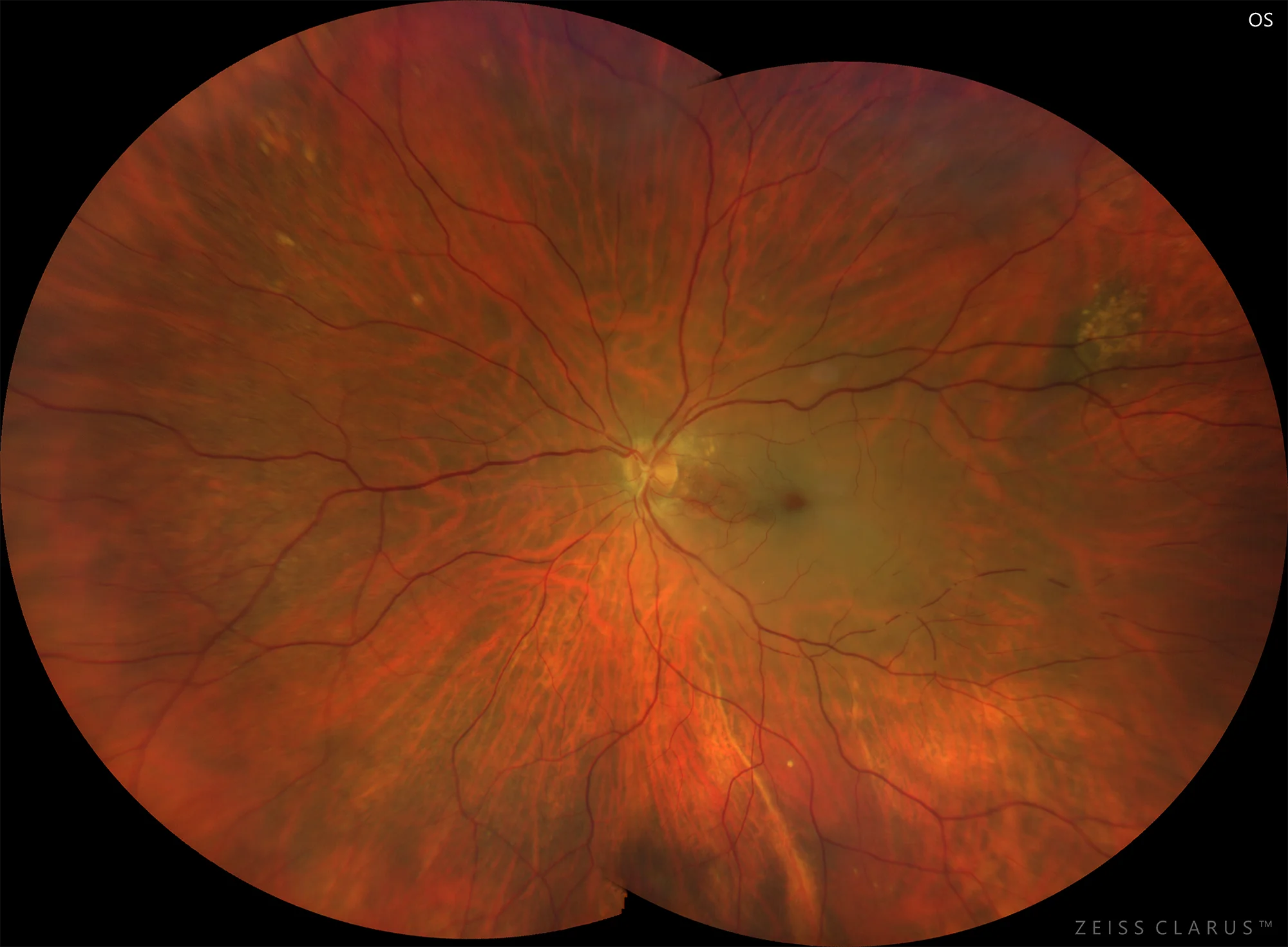
Color retinography showing macular pallor with foveal cherry red spots. In addition, segmentation of the arteries, some of which are bloodless, can be seen.
Description
Arterial occlusive disease causes retinal ischemia caused by arterial obstruction. Emboli and thromboses secondary to atheroclerosis are thought to be responsible for most cases of retinal arterial occlusion. Perivascular inflammation (as occurs in giant cell arteritis) and hypotension contribute in a minority of cases. Emboli usually form in an atheromatous plaque in the carotid artery, and because the ophthalmic artery is the first branch of the internal carotid artery, embolic material has easy access to the eye. Other cardiac causes include arrhythmias and mitral valve prolapse. Thrombophilic disorders that may be associated with arterial occlusion include hyperhomocysteinemia, antiphospholipid antibody syndrome, and inherited anticoagulant defects. Sickle cell anaemia and Susac syndrome (microangiopathy characterized by the triad of retinal arterial occlusion, sensorineural deafness and encephalopathy) are other rare causes. The signs and symptoms depend on the vessel affected by the obstruction, which, in the case of the central retinal artery, responsible for regulating blood flow to the inner layers of the retina, leads to a sudden and complete loss of visual acuity.