Best Vitelliform Macular Dystrophy
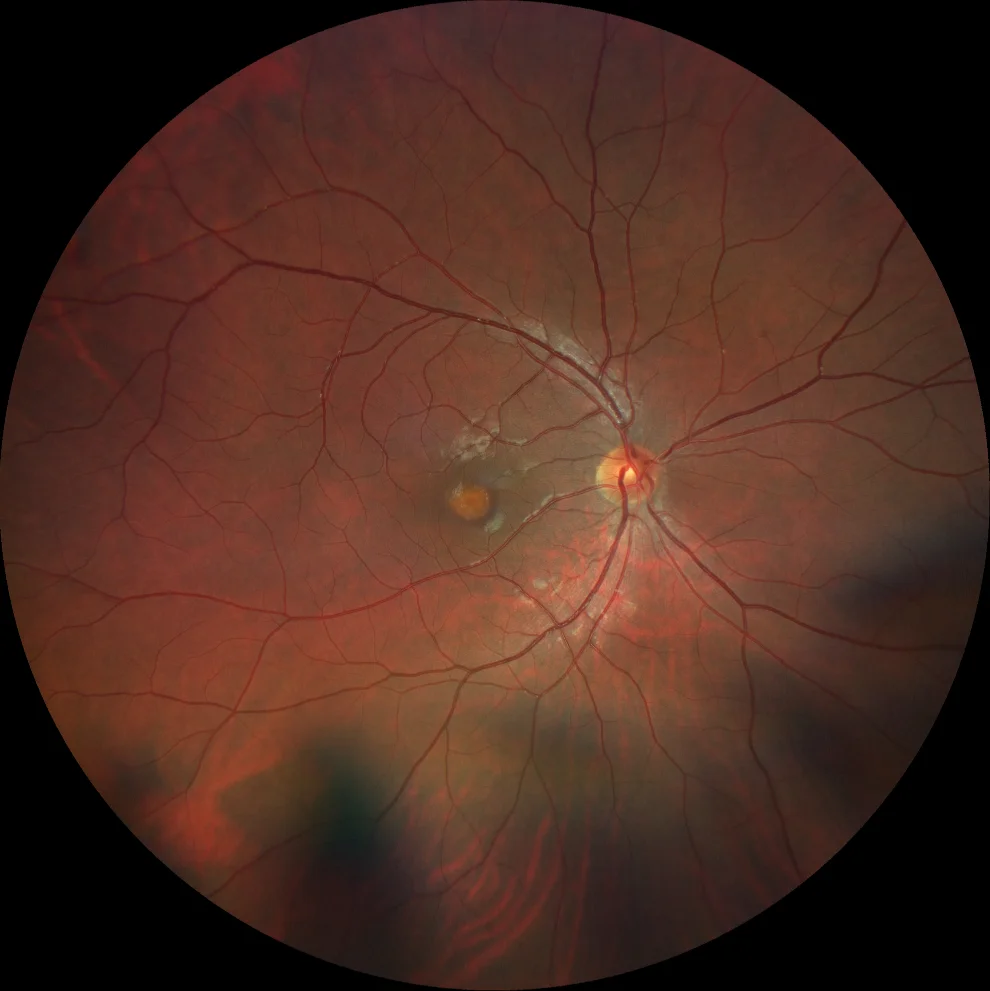
A and B. Color fundusography (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing a subfoveal vitelliform deposit, more evident in the right eye.

A and B. Color fundusography (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing a subfoveal vitelliform deposit, more evident in the right eye.

C and D. Autofluorescence images (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing hyperautofluorescence in the foveal region of both eyes, corresponding to vitelliform material.

C and D. Autofluorescence images (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing hyperautofluorescence in the foveal region of both eyes, corresponding to vitelliform material.
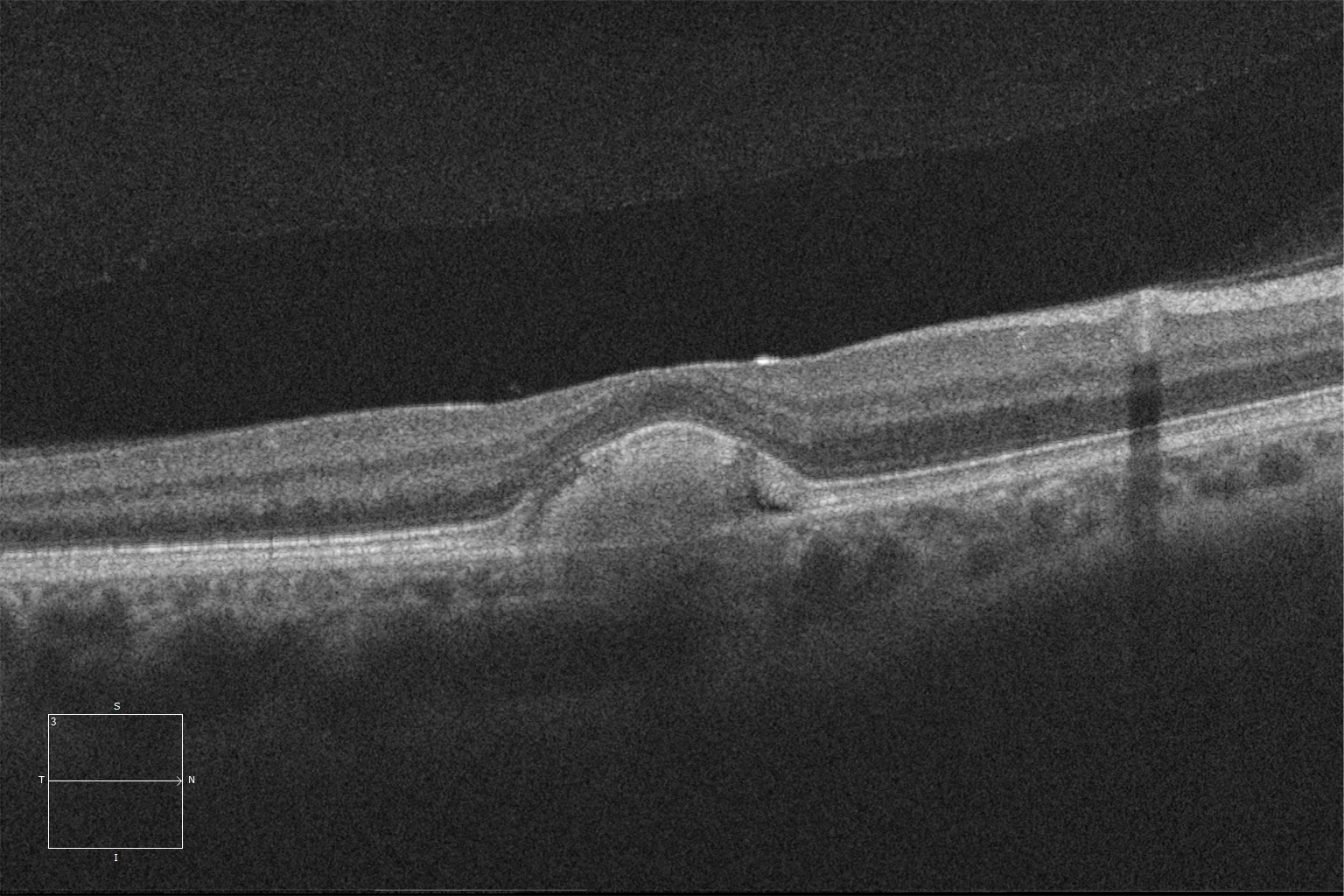
E and F. Macular HD optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing the presence of two subretinal hyperrefringent material deposits.
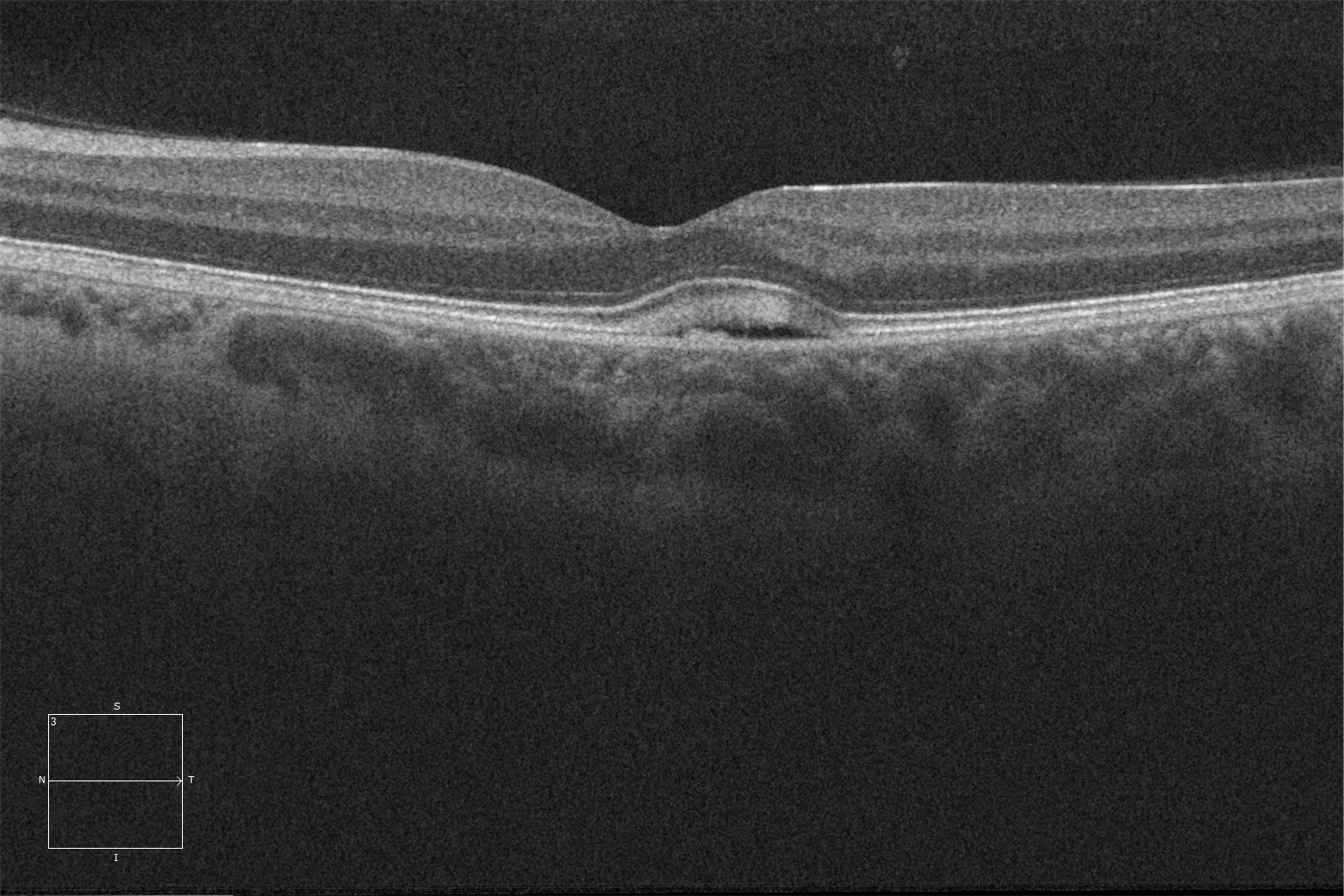
E and F. Macular HD optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing the presence of two subretinal hyperrefringent material deposits.
Description
Best vitelliform macular dystrophy is a dystrophy that affects the retinal pigment epithelium, with autosomal dominant inheritance. The affectation is usually exclusively macular, although in recessive cases there may be extrafoveal vitelliform lesions. The mutations that cause it are located in the BEST1 gene (involved in other hereditary ophthalmological pathologies known as bestrophinopathies) and present variable expressivity. The lesions are usually bilateral and appear in childhood or early adulthood. The disease consists of 5 evolutionary phases: subclinical, vitelliform (egg yolk image), pseudohypopyon, vitelliruptive and atrophic. Choroidal neovascularization appears in 20% of cases, which may require treatment with antiangiogenic agents.