Central retinal vein occlusion
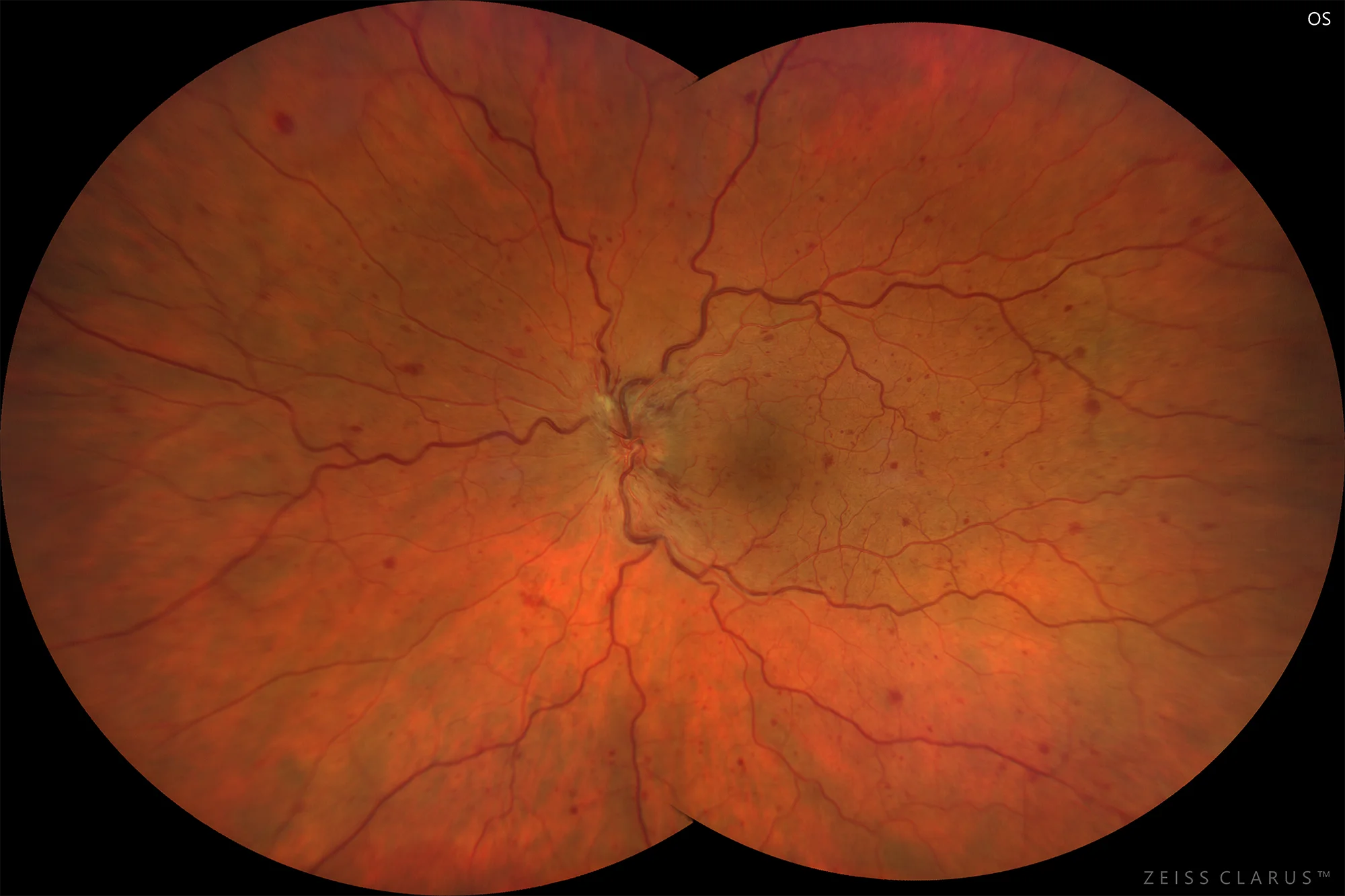
Figure 1. Color retinography showing CRVO with papilledema, vascular tortuosity, and scattered intraretinal hemorrhages.
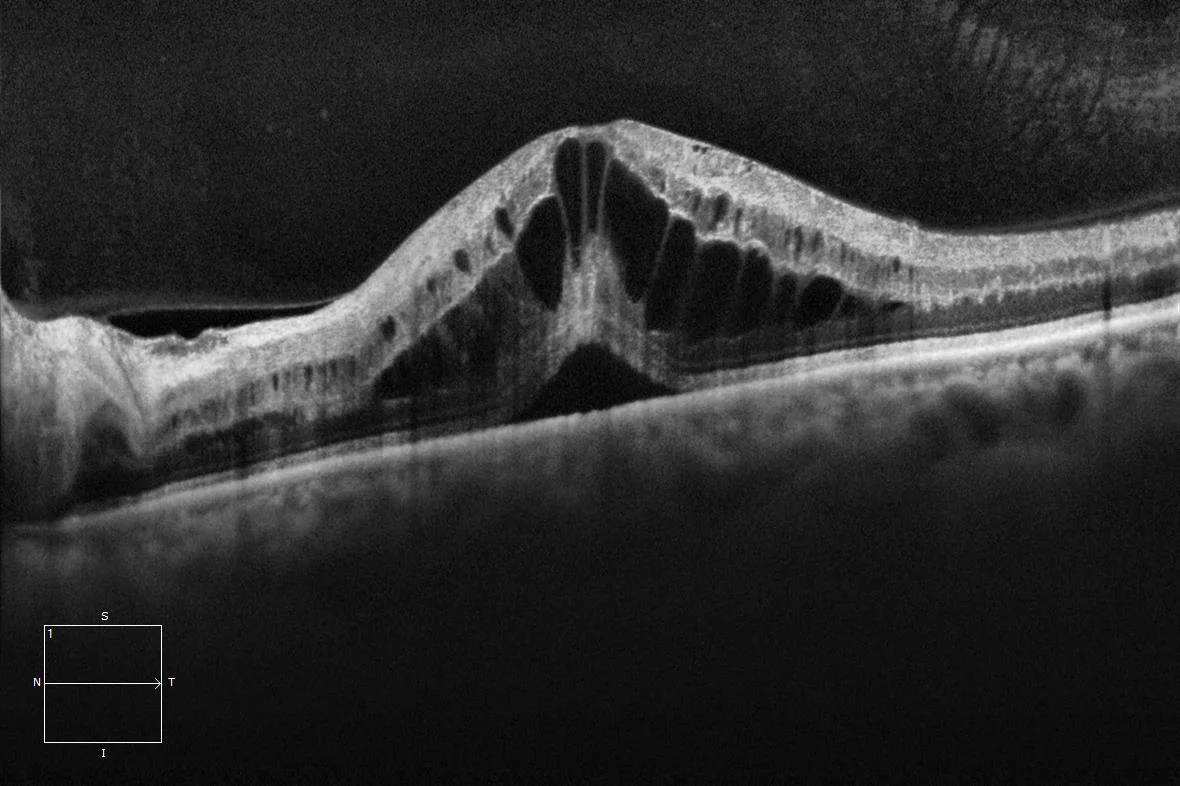
Figure 2. Optical Coherence Tomography showing cystoid macular edema and neurosensory detachment
Description
Retinal vein occlusion (RVO) is the second most common cause of vision loss due to retinal vascular disease after diabetic retinopathy. Branch vein obstruction (BRVO) is more common than central retinal vein obstruction (CRVO). CRVO is due to an occlusion of this vein at the level of the optic nerve. Thrombus formation is the primary pathophysiological factor, and endothelial proliferation and inflammatory reaction are secondary effects. Risk factors that have been associated with CRVO are open-angle glaucoma and factors such as high blood pressure or diabetes, although in patients under 60 years of age it is necessary to rule out other causes of hypercoagulability.
CRVO can be ischemic and non-ischemic, the former being less frequent but more severe in its evolution, and can lead to neovascular glaucoma and vitreous hemorrhage due to the development of neovascularization.
Macular edema is the most common cause of visual loss in CRVO, with intravitreal dexamethasone implant and antiangiogenic drugs being the treatments of choice.