Myopic Macular Hole
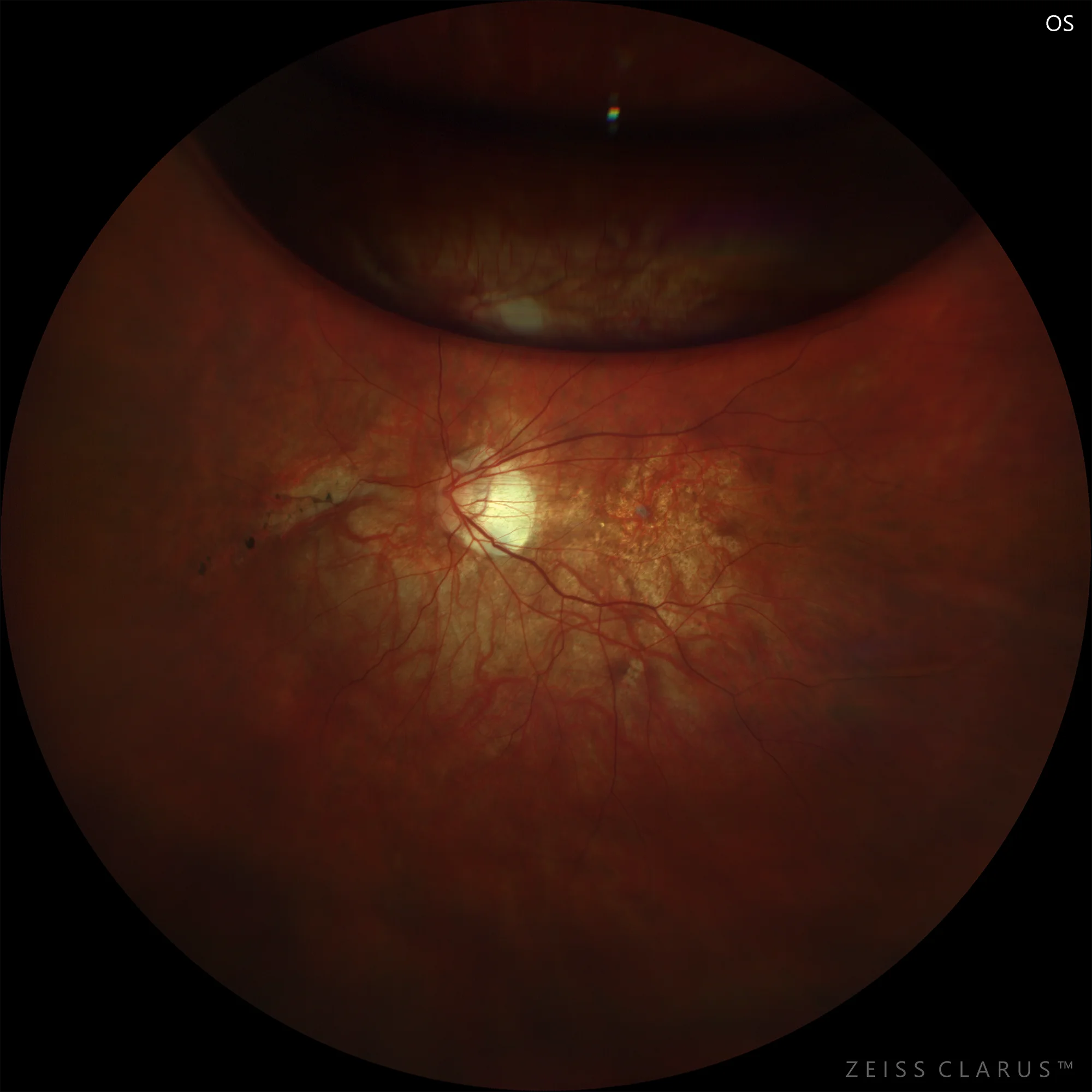
Retinography of the left eye. Postoperative, showing persistence of superior C3F8 gas bubble and amniotic membrane graft over the fovea, in the context of changes in the pigment epithelium of the macular area.
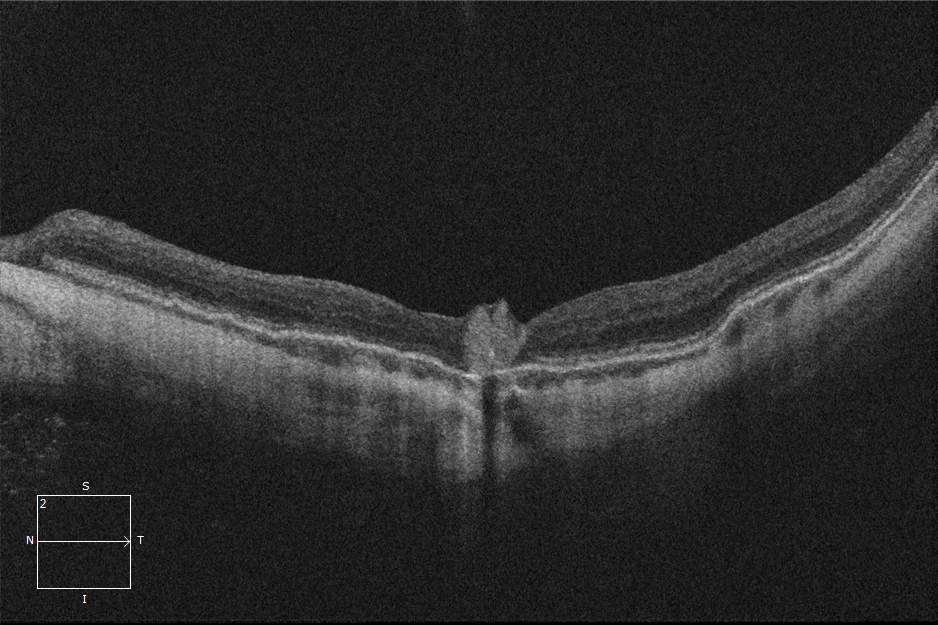
Foveal cross-section of the left eye showing the correct placement of the amniotic membrane (hyperreflective foveal deposit).
Description
Myopic macular hole (MMH) is a rare entity associated with retinochoroidal and retinal pigment epithelium atrophy, as well as the presence of posterior staphyloma, common findings in highly myopic eyes. The closure rate of MMH after the standard technique, consisting of posterior vitrectomy and internal limiting membrane peeling, is lower than that of idiopathic macular hole, with varying results according to different studies.
Although functional recovery after MMH closure may be limited in some cases, surgery is recommended to prevent the development of posterior pole retinal detachment, a frequently associated complication.