Sympathetic ophthalmia
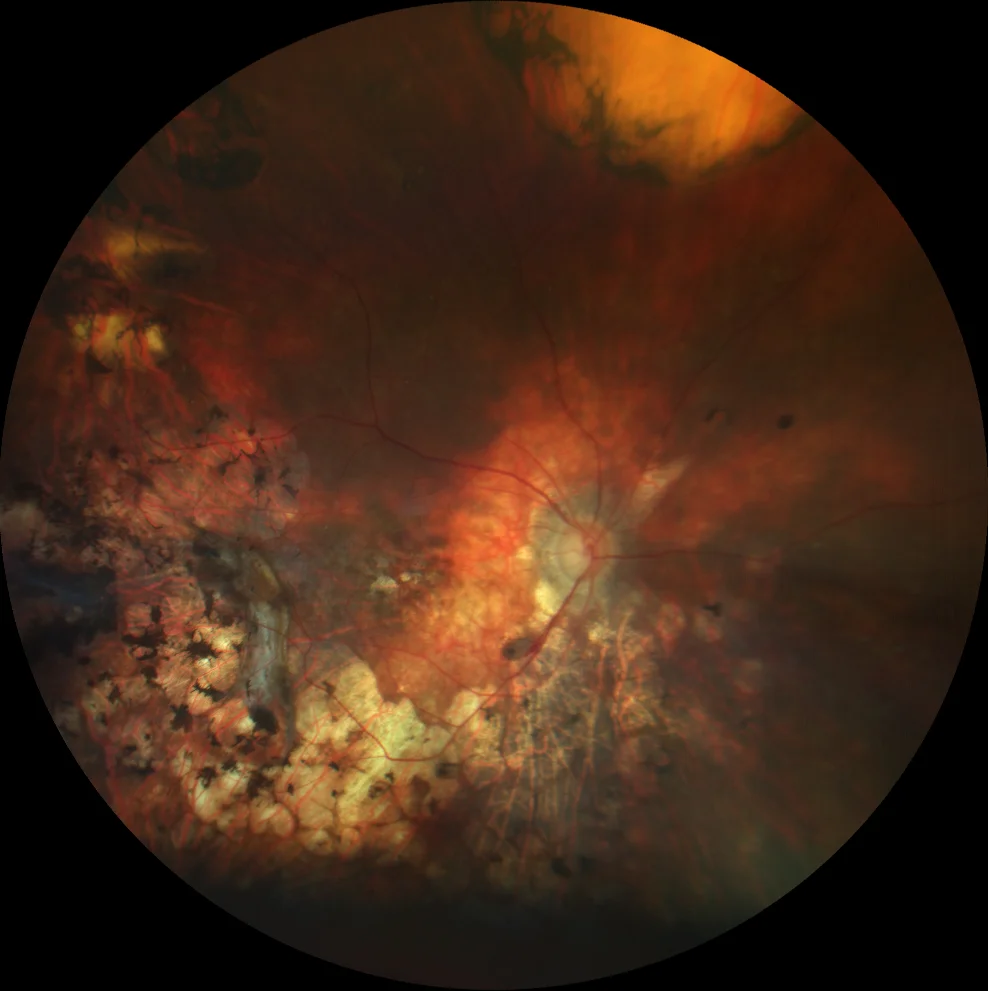
A. Color fundus graph (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the sympathetic right eye, showing a plicated retina and extensive chorioretinal scarring secondary to laser retinopexy and cryopexy.

B. Color retinography (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the left eye, showing depigmented choroidal lesions and pigmentary changes in the midperiphery.
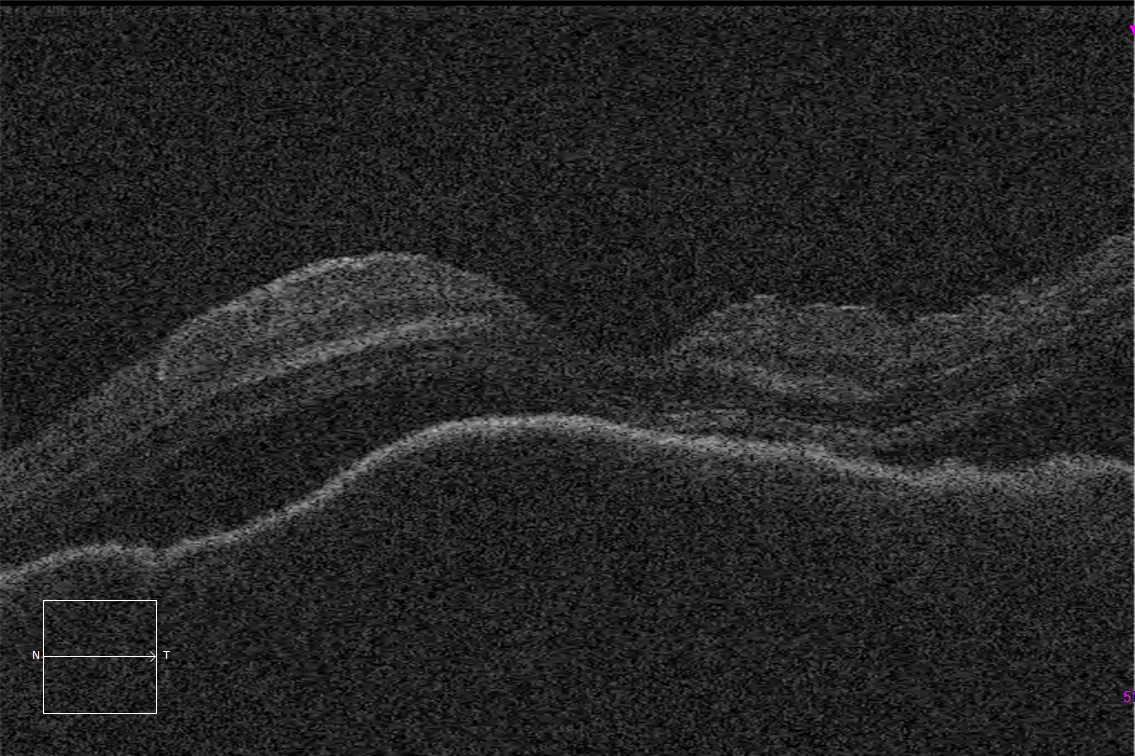
C. Optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the macular defect of the left eye in the acute phase, showing a neurosensory exudative detachment and irregular thickening of the choroid due to granulomatous inflammation.
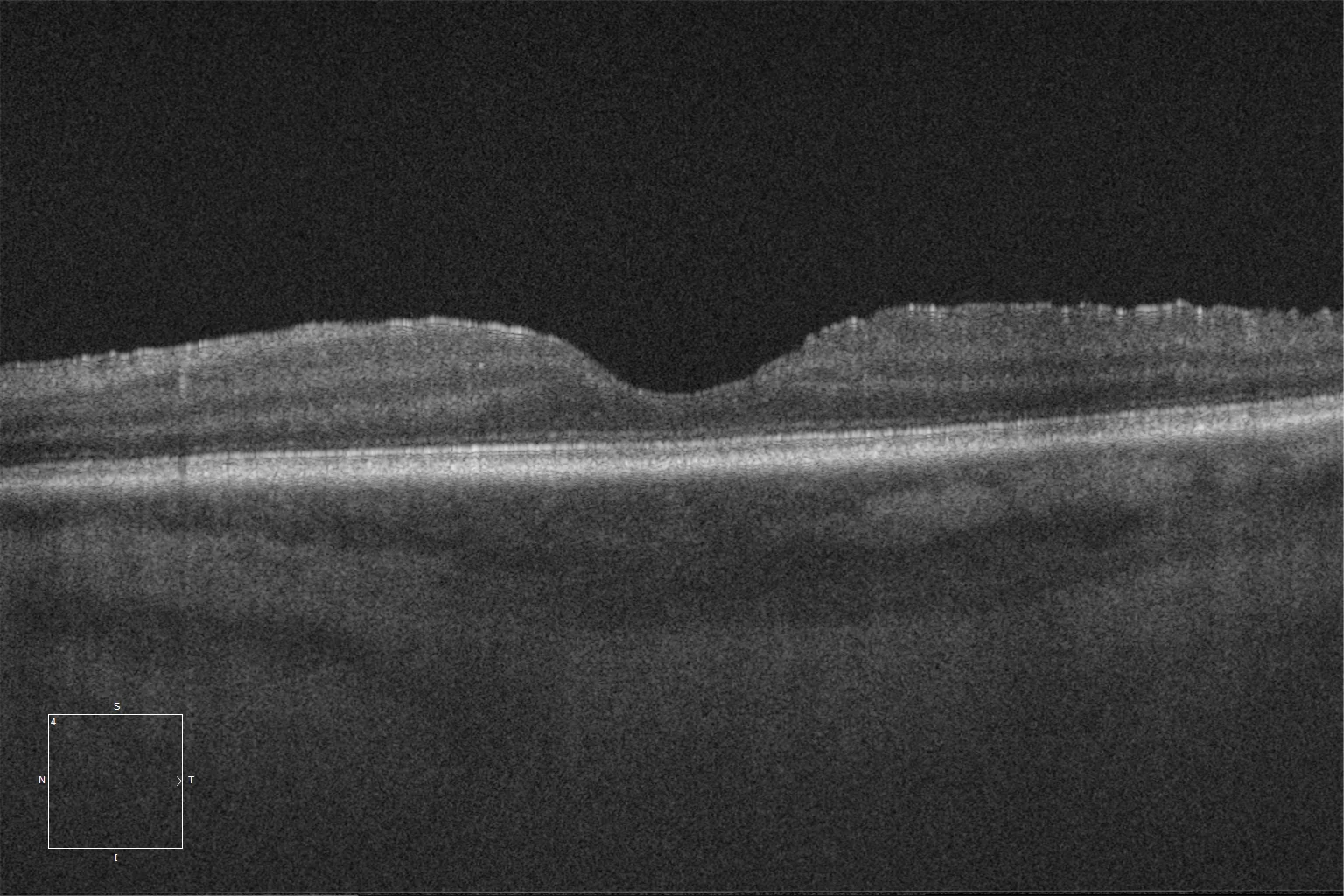
D. Optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the macular left eye after immunosuppressive treatment, showing normalized choroidal thickness, smooth Bruch's membrane, and resolution of subretinal fluid.
Description
Sympathetic ophthalmia is a rare entity characterized by bilateral diffuse granulomatous inflammation. It is produced by an immune reaction secondary to the exposure of ocular antigens after trauma or surgery in the triggering eye. Although the time of presentation is variable, it usually debuts in the first year after the traumatic event. From the clinical point of view, patients usually report nonspecific symptoms suggestive of ocular inflammation (blurred vision, photophobia, pain, etc.). The anterior segment typically presents an inflammatory reaction with granulomatous retrokeratic precipitates that may be associated with posterior synechiae. In some cases, iris thickening appears secondary to lymphocytic infiltration. Intraocular pressure may be elevated due to decreased filtration of the trabecular meshwork, or decreased due to involvement of the ciliary body. Findings in the posterior segment are variable and may include vitritis, choroiditis, optic nerve involvement, vasculitis and retinitis (although these last two are not common in isolation). A characteristic finding of this pathology is Dallen-Fuchs nodules, dispersed whitish/yellowish lesions with a rounded appearance. It is also possible to find exudative neurosensory retinal detachments (NSD) secondary to inflammation, similar to those observed in Vogt-Koyanagi-Harada disease. Optical coherence tomography (OCT) is useful to assess the presence of NSD, macular edema, neovascularization and the degree of choroidal involvement. In fluorescein angiography, the presence of hyperfluorescent points with contrast leakage at late times is common. On the other hand, in indocyanine green angiography, it is common to find dispersed hypocyanescent points. Regarding treatment, it is based on systemic immunosuppressants, with corticosteroids usually being the first choice, which should be combined with other immunosuppressive drugs for long-term control of inflammation.