Varicella zoster virus (VZV) acute retinal necrosis (ARN)
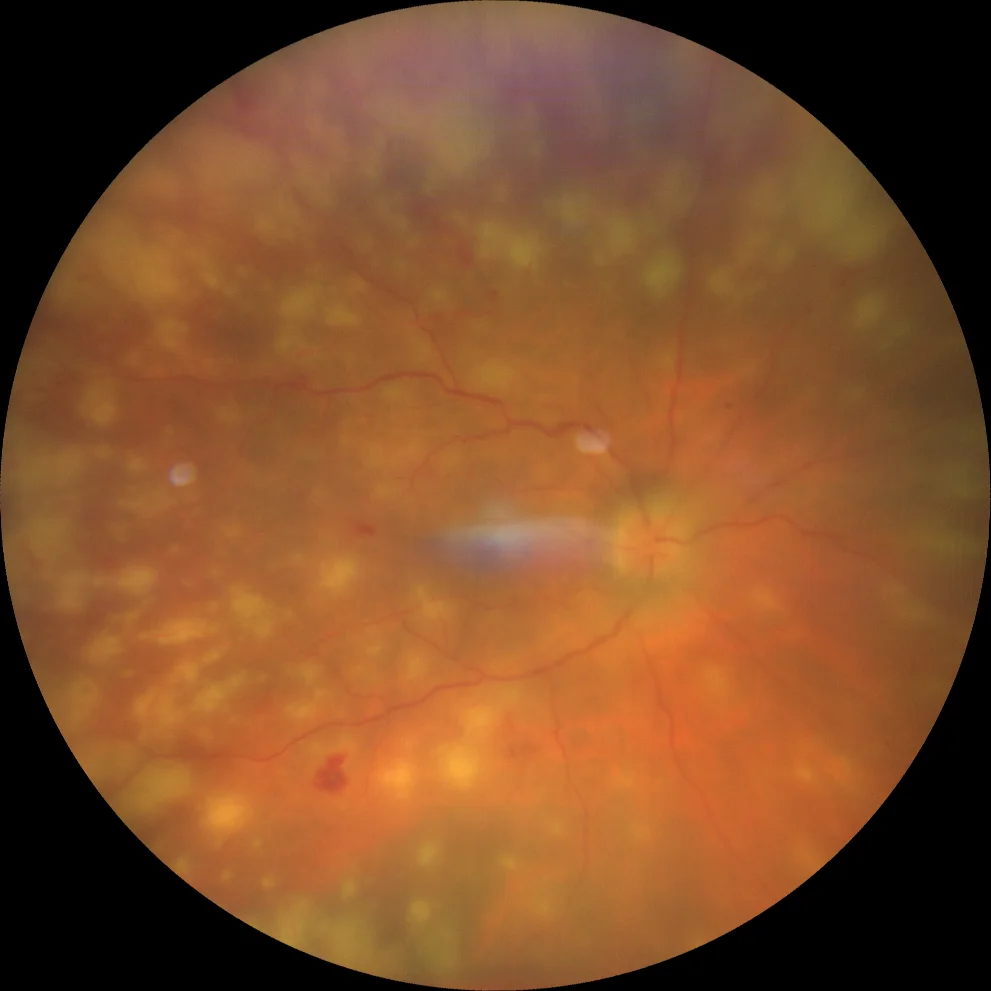
A. Color retinography (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right eye showing vitritis and multiple whitish lesions, some of them confluent, predominantly in the periphery, due to opacification of the inner retina due to ischemic necrosis induced by reactivation of the varicella zoster virus.
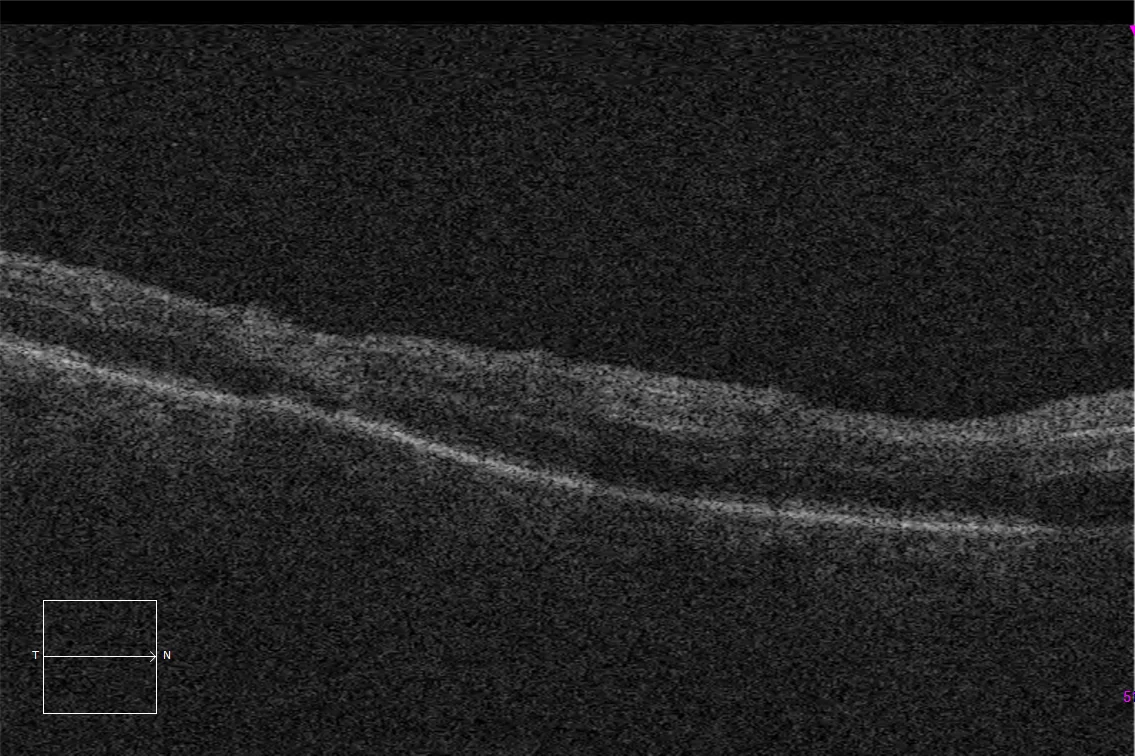
B. Macular optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) on two of these lesions, showing increased inner retinal refraction secondary to ischemia, as well as thinning of retinal thickness in one of the lesions.
Description
Acute retinal necrosis syndrome (ARN) is a rare condition characterized by necrotizing vaso-occlusive retinitis, retinal arteritis, vitritis, and often with subsequent development of rhegmatogenous retinal detachment. It is usually caused by reactivation of viruses from the herpes group (mainly VZV and herpes simplex viruses 1 and 2), and affects both healthy and immunocompromised patients.