Vogt-Koyanagi-Harada (VKH)
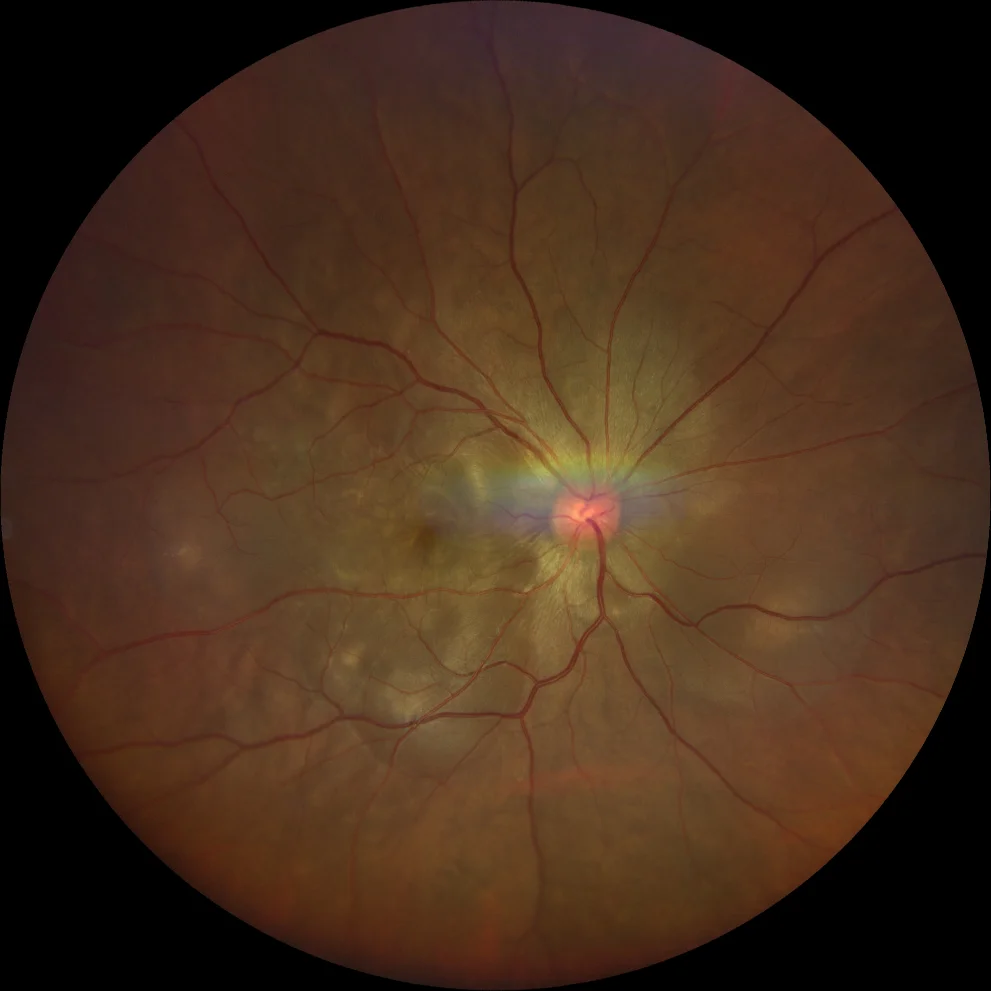
A and B. Color fundus photographs (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes of a patient with Vogt-Koyanagi-Harada syndrome in the acute phase, showing multiple exudative retinal detachments in the posterior pole of both eyes.

A and B. Color fundus photographs (Clarus 500, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes of a patient with Vogt-Koyanagi-Harada syndrome in the acute phase, showing multiple exudative retinal detachments in the posterior pole of both eyes.
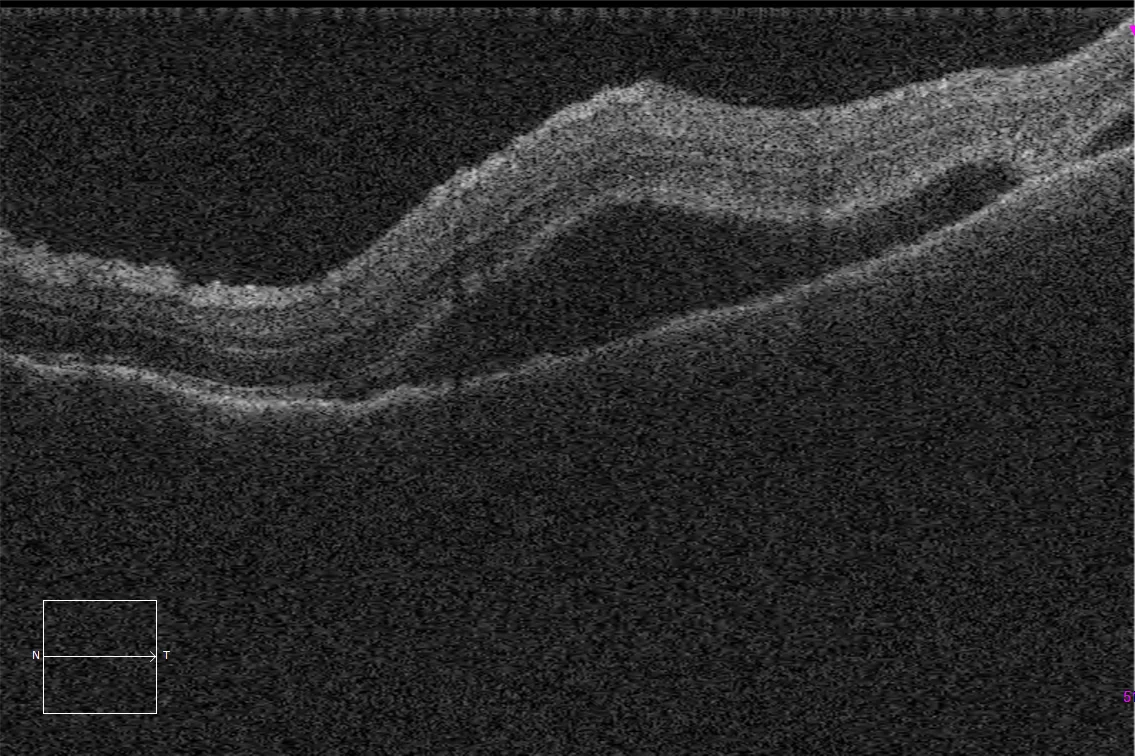
C and D. Macular optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing an irregular RPE profile secondary to choroidal thickening due to granulomatous inflammation, together with septate bacillary detachments, characteristic of Vogt-Koyanagi-Harada syndrome.
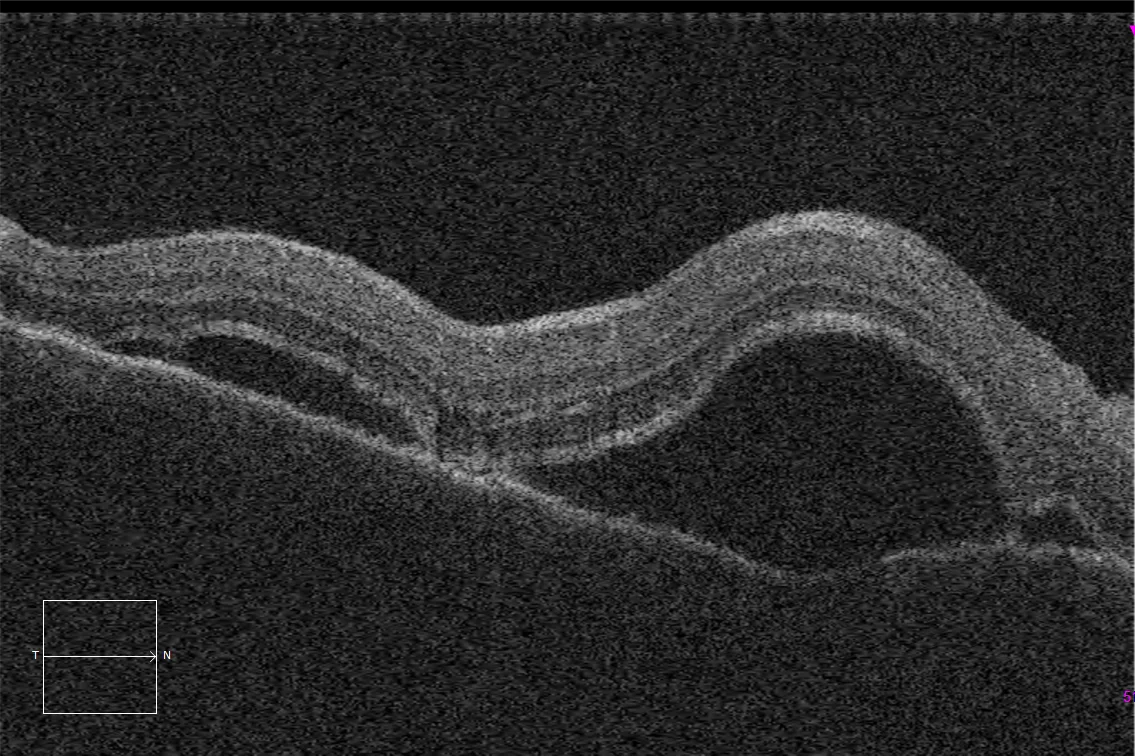
C and D. Macular optical coherence tomography (Cirrus 5000, Carl Zeiss Meditec ASG, Jena, Germany) of the right and left eyes, showing an irregular RPE profile secondary to choroidal thickening due to granulomatous inflammation, together with septate bacillary detachments, characteristic of Vogt-Koyanagi-Harada syndrome.
Description
Vogt-Koyanagi-Harada (VKH) syndrome is a multisystem disease presenting with a combination of ophthalmologic, neurologic, and dermatologic signs and symptoms. The main clinical finding of VKH is bilateral granulomatous panuveitis. Cutaneous features include vitiligo , alopecia areata , and poliosis , and neurologic features include meningismus, hearing loss, and tinnitus.